Introducing the Five Giants.
Learn about all five of the giants and our summary policy asks here.
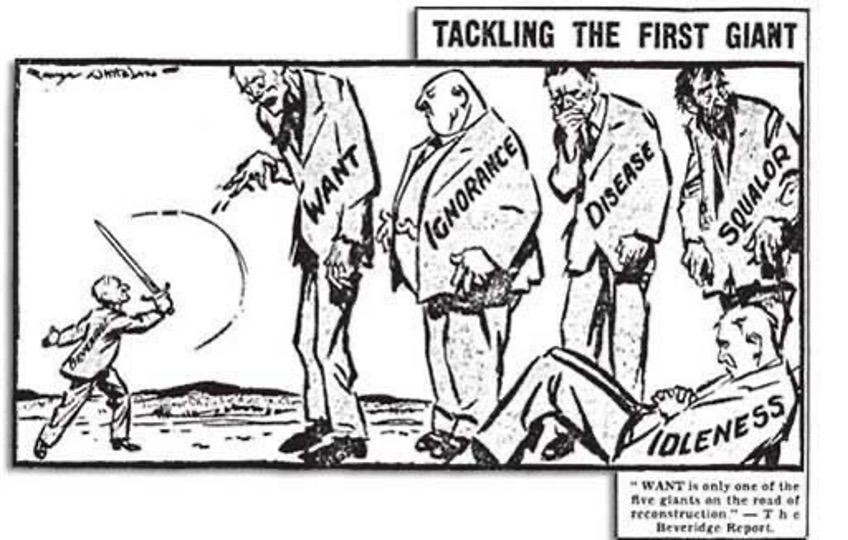
Who are the Five Giants?
The Five Giants are:
Housing, sanitation and the environment
Unemployment
Poverty
Health and social care services
Education
The Five Giants are the key factors will determine the life chances and opportunities for any individual person. They are known as the social determinants of health. Eventually, they will determine who develops a disability early, and who dies early.
Often these days, the social determinants of health are summarised as smoking and obesity. This is inaccurate, because smoking and overeating are addictions, health conditions which result from the social determinants of health, not the social determinants of health themselves.
Desmond Tutu explained this difference well:
“There comes a point where we need to stop just pulling people out of the river. We need to go upstream and find out why they're falling in.” [i]
If we go upstream today, we will find it is the Five Giants pushing people into the river, making people ill from all kinds of physical and mental health conditions. We need to urgently stop them.
History of the Five Giants
The Five Giants were first recognised officially by the government in the 1937-1939 Welsh TB Inquiry.
This was because of the compelling statistical evidence on higher TB deaths in Wales provided by UK friendly society leader John Tomley, who was responsible for most of the UK’s healthcare for workers at the time. He had also helped found the first ever national health service pilot in the UK, for TB in Wales.
John Tomley’s great-granddaughter, Emma Snow, has recently rediscovered John’s work. This was after Emma had already developed her own professional interest in the Five Giants, as a charity CEO supporting unemployed people with disabilities. She has written a book about John’s work fighting the Five Giants, her own experience as a charity and NHS worker fighting the Five Giants, and as a person with a disability, facing early death herself. This inspired her to set up our new people powered think tank, the Five Giants Foundation, with a group of other people with disabilities, some of whom are facing early death, carers, and professionals. Our aim is to help people learn more about the Five Giants today, and how to fight them effectively.
Back in the 1930s, John Tomley campaigned for many years for a government inquiry and the recognition of how the Five Giants determine our health. In 1936, he asked:
“Are we to act fearlessly and effectively as a Fire Brigade in extinguishing the conflagration, or are we content to be merely a Salvage Corps dealing with the debris and the ruins, instead of fighting the living and devastating flames?” [ii]
John’s campaigning finally led to the Welsh TB Inquiry. In this government inquiry, the leaders of the inquiry, Dr Francis Coutts and MP Clem Davies, surprisingly stepped outside the official boundaries of the inquiry set by the Minister of Health, just as Lord Darzi has done in his recent report on the NHS in September 2024. Like Lord Darzi, they widened their scope to include the whole of the Five Giants.
Unlike Lord Darzi, who has only had time to conduct a rapid review of the NHS, the leaders of the Welsh TB Inquiry interviewed patients, doctors and nurses across Wales for two years. As the giants were running wild at the time, it was possible to find them from death statistics between different areas and groups of people. They found that:
People with poor housing, sanitation and environmental conditions died earlier
People who were unemployed died earlier
People on lower incomes died earlier
People without health and social care services died earlier
People with less education died earlier
People who had one issue were more likely to have the other issues. The effect of the Five Giants was not just confined to the person themselves, but also caused their families to die earlier.
All this evidence of the Five Giants led directly to the Beveridge Report and the setup of the NHS and modern welfare state. When this was first set up by Nye Bevan, Jim Griffiths and others in 1948, it was with one purpose in mind: to fight all five of the Five Giants. This would mean that everyone could live healthier, happier and longer lives. Government departments were set up to fight each giant.
The Five Giants today
Yet, since 1948, our success fighting the Five Giants meant that we became complacent. As the giants faded from many people’s lives, and most people no longer had to face early death, we forgot about the existence of the giants. So when we wanted to save money in austerity, we took away the infrastructure we had built to guard against their attacks, as we believed it was no longer relevant.
Yet this has had very expensive results. Once one giant has attacked, the others tend to attack too. Helping people after they have already been attacked by the giants and developed ill health is far more expensive than preventing the issues that made them ill in the first place. “A stitch in time saves nine”, the saying goes, and the NHS is now having to do the nine stitches instead of prevention having to do one stitch. This is why we all urgently need to understand the Five Giants today.
To many people, the issues facing Britain and the wider world have become more complicated in recent years. Rising inequalities have created tensions in society. Economic swings still plague households with uncertainty and volatile living standards. The recent experience of the Covid-19 pandemic reminds us of the interlinkages around the world, and also human fragility. Global warming and the environment is arguably the biggest issue of modern times. And sadly, war and conflict continues to destroy the lives of too many people and deprive others of home, hope and opportunity – too much wasted human potential. But these are macro issues, which impact at that scale.
The Five Giants impact, most tellingly, at the micro level. Each individual is at some point touched by some, if not all, of these headings in a way that impacts them very directly. For many people all five of the Giants have a direct impact in their daily lives. These are in essence the timeless yardsticks of social policy that resonate down the centuries. We need to measure our current efforts against them. Life in Britain is better than 100 years ago, but in many ways worse than 1948. Inequality and unfair lack of opportunity is still with us, and has grown in recent decades, particularly since austerity. Much more could be done to give all people the opportunity and freedom we all seek, but which can be constrained by disadvantage, as described by the Five Giants.
Over the years policy has sought to address these inequalities and must continue to do so. The objective must be to push the boundaries of each area and use the measure of these giants as the challenge of our times.
Lord Darzi review
The latest review of the NHS by Lord Darzi has just been published, in September 2024. Lord Darzi has, unusually, used his review to mention health issues which were outside the official scope of the review, the Five Giants. This mirrors times in the past when leaders of government inquiries chose to widen their own scope, most notably the Welsh TB Inquiry 1937-1939, where the MP and doctor leading the inquiry felt compelled to include the Five Giants.
Lord Darzi’s report tells us:
”The state of the NHS is not due entirely to what has happened within the health service.
The health of the nation has deteriorated and that impacts its performance
Overall life expectancy increased in the 2000s, but plateaued during the 2010s, before decreasing during the Covid-19 pandemic. It has started to rise again now, but the absolute and relative proportion of our lives spent in ill-health has increased.
Many of the social determinants of health – such as poor quality housing, low income, insecure employment – have moved in the wrong direction over the past 15 years with the result that the NHS has faced rising demand for healthcare from a society in distress.
There has been a surge in multiple long-term conditions, and, particularly among children and young people, in mental health needs. Fewer children are getting the immunisations they need to protect their health and fewer adults are participating in some of the key screening programmes, such as for breast cancer. The public health grant has been slashed by more than 25 per cent in real terms since 2015 and the country’s main public health institution was abolished – split into two new bodies – in the middle of the pandemic.”[iii]
Lord Darzi’s historic intervention is our once-in-a-generation indication that, once again, the time has come for us to fully understand and tackle the Five Giants.
Systems Thinking
From our experience as service users, carers and frontline service delivery professionals, we believe that a Systems Thinking approach should be adopted to fixing complex social issues across the Five Giants. Systems Thinking means better outcomes for less money. It is a way of solving complex social issues, using the smallest amount of money and other resources.
Effectively, the original founders of the NHS and welfare state in 1948, including Nye Bevan, Jim Griffiths and others, were using Systems Thinking when they focused on health prevention through the Five Giants, although the term Systems Thinking hadn’t been invented yet. Their knowledge was simply from having long experience of the issues and trying different ways to tackle them over many years, to find out what works.
Systems Thinking was originally developed by Donella Meadows for engineering and the environment,[iv] and then adapted by David Peter Stroh for social issues in the USA.[v] It is now in use by government, including the public sector. For example, the NHS local commissioning groups, Clinical Commissioning Groups (CCGs), became Integrated Care Systems (ICSs) in 2022. The word “System” is used in the ICS name because of Systems Thinking: there is an intention to use Systems Thinking to improve care. Yet, because of the current pressures on the NHS, Systems Thinking training has not yet been rolled out to staff and patients. Through these policy papers, we intend to show examples of how Systems Thinking can be applied to the UK public sector and its partner organisations.
Fully putting Systems Thinking into practice across the public sector would mean that people who have experience of the issue should be the key participants and facilitators of a Systems Thinking group of eight to ten people to solve the issue, as well as the different frontline staff involved in supporting them across the public sector and voluntary and community sector, and the government leaders making decisions. Vicious circles can be looked at, and points of leverage found where there is a strong business case because the application of a relatively small amount of resources saves a lot more resources further down the line.
Summary of Five Giants policy asks
We have created a policy paper for each of the Five Giants today, covering the key issues facing us now, and setting out detailed business cases.
Many of the issues which face us now were solved in the original 1948 NHS and welfare state model, set up by Nye Bevan, Jim Griffiths and others. Our first priority must be to look at what worked well and was cost effective in the past, and avoid reinventing the wheel.
Many of the measures which worked well in the past were set up due to identifying the causes of huge numbers of people dying early in the 1920s and 1930s, from pandemics, to young people dying of TB, to mothers dying in childbirth. People like Nye Bevan’s own father, who died of a lung disease caused by being a miner.
Nye Bevan and Jim Griffiths promised that their deaths would never be forgotten, as we would use this learning to create a new NHS and welfare state which worked for the many, not just the few, and avoid similar deaths in future. Yet, during austerity, tragically we have forgotten this hard won knowledge, and scythed away the welfare state too far. As a result, for the first time since 1948, people have started dying earlier. We must urgently reverse this, by putting back what works.
Nye Bevan and Jim Griffiths knew that prevention is always cheaper than cure, and made sure that prevention was always prioritised across the NHS and welfare state when it was first set up in 1948. This meant most people did not develop health issues in the first place, avoiding costly NHS care. Where a person needed low cost care, such as social care in their own home, they would be given it free in order to avoid a more expensive hospital admission. Overall this was found to save money. Yet during austerity we have forgotten about prevention, and that is a key reason the Five Giants are starting to run wild again today.
There are also some areas where new challenges and new opportunities have arisen since 1948, particularly with environmental challenges and digital opportunities.
Below, we summarise the key policy asks resulting from our detailed policy papers on each of the Five Giants, also available here.
Giant 1: Housing, sanitation and the environment
“Enough land to build houses for everyone on the UK social housing waiting list could be bought for less than £14 per head of population.
Counterintuitively, the biggest factor in health is not health or social care services at all, but housing and sanitation. Therefore social housing must be our first priority now in reducing early death, followed by recommendations in our other policy papers to fight the other Five Giants.
A Systems Thinking approach can help us understand the issue further. Looking at points of leverage, we find that the cost of housing is made up of three parts: the cost of land, the cost of the building, and the cost of infrastructure. There are lower cost options for all three, particularly the cost of land.
Land costs to house the entire UK social housing waiting list could be slashed to £14 per head of population. This is by using the original 1948 welfare state model of the government buying low cost land which does not yet have planning permission, then granting planning permission afterwards, and abolishing hope value from compulsory purchase of undeveloped land.
Even if we had to use only farmland for new housing, it should be possible to build social housing to house everyone on the social housing waiting list on 0.14% of the farmland, and still have plenty left over for farming. Yet there are also other types of land which could be built on, such as former airfields, car parks, petrol stations, military land, and the plots of surplus university buildings. Larger sites which have already been built on once should therefore be prioritised for new social housing first.By building new homes in bulk, we can add infrastructure such as new sewerage facilities for the whole area. This is cheaper than the current piecemeal development of homes in every local area, which costs more because it means a larger number of existing sewers across the UK will get overloaded and all have to be replaced.
The Beveridge Report giant of housing and sanitation also included the environment. On the subject of the environment, by building new homes within walking distance of existing train lines, we can add new train stations within walking distance of all homes, and put on more regular trains. This is much cheaper than building new train lines. The cost of using the train also needs to be made cheaper and easier than car use, through unlimited free parking at train stations and very low cost train tickets, funded by a vehicle tax per mile, chargeable through an onboard box in the car. Train lines also need to be electrified, to reduce pollutants in nearby homes. Car use in urban areas could be restricted when there is high pollution.
In this way, we can provide affordable, healthy social housing for all, at a reasonable cost, and have a major impact on health inequalities.
Giant 2: Unemployment
“There is a very clear business case to invest a significant amount in supporting people who are likely to return to work. Public Health England has found that, for each person who returns to work, there is a net benefit to the government of £12,000.”
After housing, the biggest factor in health is again not health or social care services, but unemployment. This is because people remaining in employment both helps prevent early death for the person and their family, and also means they are contributing to the costs of the NHS and wider welfare state, through taxes. Therefore reducing unemployment must be our second priority now in reducing early death, after housing.
The majority of long term unemployed people have at least one disability. This means we need to prioritise reinstating support for unemployed people with disabilities.
First, we need to prioritise prevention: preventing people becoming unemployed due to a disability in the first place, primarily through tackling the Five Giants, ensuring decent work at Living Wage or above is available, and slightly prioritising working age people in NHS services, so that they are not stuck on NHS waiting lists which cause them to become unnecessarily unemployed.
Next, we need to rebuild the disability employment support which used to be funded by the DWP in the past. This needs to cover all stages required for most unemployed people with disabilities to return to work, in a logical order. This should start by helping people get the medical treatment they need, and giving them sick pay so that they can recover effectively from their illness. Then it should go on to disability specific employment advice and job matching, as well as retraining and work experience where necessary.
Finally, there needs to be a focus on creating jobs which can actually be done by people with disabilities. Local disability employment advisers can help employers such as health and social care employers to restructure their roles with job carving, so that people with disabilities can help to fill their many vacancies, in particular through enabling flexible and home working.
For people with disabilities who still remain unemployed, subsidised employment should be reintroduced. The models that have worked in the past are slight overstaffing of entry level roles in the public sector, and the Remploy and Women’s Home Industries model of subsidised organisations set up to employ people with disabilities to make items. Ideally the options would include working from home as well as on site, as working flexibly from home is the main need for people with disabilities who are unable to work for mainstream employers.
In this way, we can do our best to fight off Unemployment, the second of the Five Giants, and fund the NHS and wider welfare state to fight off the other giants.
Giant 3: Poverty
“If we want to reduce health inequalities, then the most obvious way to tackle this is through reinstating the key 1948 welfare state measures to reduce the effect of poverty, which worked in the past. Ironically, this is also likely to be cheaper than the current patchwork of services which have sprung up to reduce the effects of poverty, such as food banks.”
The third of the Five Giants, Poverty, often attacks alongside Housing, Unemployment and Health. Poverty leads to immediate health issues, such as not having enough healthy food to eat, leading to malnutrition, a key cause of preventable hospital admissions. Therefore reducing poverty must be a top priority now in reducing early death.
Being on too low an income is actually known to reduce brainpower, where people have so much of their brain taken up by worry that they are unable to use their brain to make good life choices for themselves and their children. In order to enable people to make healthier choices, all benefits should therefore be adjusted to reflect people’s actual living costs, and benefits caps should be scrapped. Instead, enough affordable social housing should be built so that people in work can earn enough to cover their living costs, without needing to rely on benefits.
People with disabilities should be supported with enough benefits to recover and return to work if possible.
Reasonable mortgage costs should be funded with housing benefit, if they are lower than rent, to avoid forced home moves when people become ill or unemployed.
Working age adults should be allowed to keep their savings and claim benefits, which is the situation for pensioners.
Subsidised food, free school meals, free community meals and free meals on wheels should be reintroduced.
Trauma should be treated by eye movement desensitisation and reprocessing (EMDR) being made available on the NHS, to prevent the trauma and poverty cycle passing to the next generation.
Young people should be allowed to stay in their family home when their parent goes into care or dies, rather than forcing them to sell or leave their family home where they have memories of their parent. This is currently a leading cause of youth homelessness.
Benefits being too low is currently a key driver of crime, like in Victorian times. Where people are unable to survive on benefits, people feel justified in breaking the law, and other people feel this is fair enough. Benefits which cover living costs, for everyone in the UK, therefore contributes to the rule of law being respected and followed by everyone.
Giant 4: Health and social care services
“By using Systems Thinking, we can first focus on areas where we can prevent the need for a hospital appointment entirely, saving 100% of each appointment time. This is called effectiveness. When prioritising our actions, it is better to focus on effectiveness first rather than efficiency, because it saves a lot more money. After that, once our services are effective, we can spend time tweaking efficiency to make each one as efficient as possible too.”
The biggest factor in health is not health or social care services at all, but all the Five Giants, the social determinants of health. Prevention is also much cheaper than cure. Therefore fighting the full Five Giants with prevention must be our first priority now in reducing early death.
Yet there is still plenty to do in health and social care services. We need to optimise effectiveness first - preventing a need for a service in the first place - and then efficiency - making each doctor’s appointment slightly quicker with, for example, improved digital systems or medical equipment.
A Systems Thinking approach can help us understand the issues further.
This shows us that funnelling more money to A&E takes it away from areas that are already underfunded, such as prevention, self management and home care, as there is a fixed pot of money in total. These other areas are much cheaper per person saved from early death compared to A&E. Therefore the other areas should be prioritised first.
Prevention needs to encompass both the Five Giants in general, and ways to prevent specific diseases, such as fully funding PGD IVF to eliminate genetic diseases from affected families, where there is a strong business case.
After we have used prevention to reduce the need for GP appointments in the first place, GP services need to be restored to the appropriate level, so that people can see their GP on a timely basis and not have to go to A&E. NHS dental care should also be urgently reinstated across the country. GP and district nurse home visits also need to be reinstated, as currently many people needing a home visit are told to go to A&E instead, which is much more expensive. For most people, they will recover quicker at home in their own bed, rather than in hospital.
Next, for hospital appointments, there is often a long waiting list.
People aged under 67 should be slightly prioritised, as this helps them go back to work quicker, so they can pay more tax, in order to fund the NHS more for older people. This also improves health equity, to reduce the rising trend of early deaths. People with any disease that could result in early death should also be prioritised, not just cancer.
Currently, for administrative reasons, if people need to be seen by another doctor at the hospital, they are referred back to their GP. Many people have to be re-referred multiple times for the same issue, causing them multiple waits, extending to many years. This is particularly an issue with autoimmune conditions, a top 10 killer for women, and a key cause of early disability. This should be urgently tackled and people should only have to wait once.
Hospital teams should also be able to organise themselves more effectively, including enabling patients to see multiple staff in one visit, restoring the option of inpatient stays for people with complex medical conditions which are difficult to diagnose, and enabling more generalist doctors in hospitals, who can look at patients with symptoms in more than one of their body systems.
Originally, in the 1948 welfare state model, social care was free. Yet this has been eroded over the past decades, and adults with disabilities now have to pay for social care, such as care homes and home care. Social care payments do not work well, because they cause delays in people leaving hospital. They are unfair, because people who have had good legal advice can often avoid the payments. People are also financially incentivised to remain in hospital if they can, even though this is much more expensive for the taxpayer than free social care would be. Instead, social care free at the point of use should be reinstated, primarily funded by savings from the reduced number of bed days in hospital. Our Systems Thinking game demonstrates that this is cheaper for the taxpayer.
Social care payments were designed for older people. They are particularly unfair for people dying early below age 67, leaving their children without savings, evicted from their homes by the state, and at high risk of homelessness. Social care payments should be immediately stopped for the small number of people dying early below age 67, as this is a low cost tweak to the current policy which immediately helps tackle the leading cause of youth homelessness. Any children still living at home should be treated as dependants, no matter their age, and should be allowed to continue living in their family home.
Death is not well catered for in the NHS, as the NHS was designed for saving lives, even though the vast majority of people in hospital beds are frail older people who will die relatively soon. Instead, hospice at home and hospice ward services should be developed. Hospice care should be fully funded by the NHS, as it is cheaper than hospital. Relatives should be given support and a keyworker immediately at every death. Post mortems should be speeded back up to take 24-48 hours, to prevent delays in funerals causing issues with employers.
Mental health needs strengthening. Psychological trauma is a key way that the Five Giants affect families from one generation to the next. One person dies early, and this then causes trauma to their family members, making them at higher risk of early death themselves. Breaking the cycle involves prioritising acting on the Five Giants to prevent traumatic events in the first place. For people affected by trauma, the new effective EMDR treatment should be made available to patients on the NHS, as this saves a lot of resources further down the line.
The definition of Adverse Childhood Experiences (ACEs) used by social care should also be updated to include the most traumatic experience: disability or death of the child or their parent. Currently this has been omitted from ACEs. This means the most vulnerable group of children and young people will be covered and can be prioritised for support once again. Overall, social care for children and families should also be restored to at least pre-austerity levels of staff, funding and services, including all the services that social workers need to refer people to. The current postcode lotteries should also be fixed, so that everyone has a decent quality of local services relatively close to home.
Staff vacancies are high, and this affects the ability of the NHS and social care to provide effective care. Nurses are particularly affected by student loan repayments, which do not take into account costs of families. A funded college HND would be equivalent to the second year of a university degree at lower cost. This could form the standard nursing qualification. Nurses could then top it up to a degree by doing a third year at university if they want to be promoted above a certain level. The full qualification should be paid for upfront by the employer.
Meanwhile, carers are paid very low effective rates due to not being paid for travel. The local council taking over care again, and arranging for each carer to support patients in the same few streets, would cut down on travel and enable each carer to serve more people. We have also created a new Integrated Care System (ICS) wide strategy game to model the effect of paying carers the market rate, by increasing pay from £15 per hour to £17 per hour for all carers. This shows that, when the saving in hospital care is taken into account, there is an extra cost in Year 1, followed by a saving from Year 2 onwards. In total there is a significant net saving over 5 years.
Overall, this illustrates the general issue that accounting is often perverse in NHS; cutting back in one area of healthcare can have huge consequences on other areas. This means that managing budgets and contracts for separate local health and social care organisations, each with their own management team competing with the other organisations’ management teams for funding, can often make patient outcomes worse rather than better. Instead, merging all local health and social care into one organisation for each Integrated Care System (ICS) area would be much better for patients. The organisation could then have one overall goal of reducing early death and early disability below age 67 for the whole local population.
Finally, on digital, a full shared NHS wide database should replace the current limited information on the NHS Spine. This would mean accurate information can be seen by all doctors, nurses and other professionals at every appointment, enabling patients to be treated quicker, and reducing medical errors. A physical on site backup of local patients’ records should be kept on local computers in hospitals and GP surgeries. This means that if the cloud systems are down, there are still patient records to cover the majority of patients. Systems Thinking also shows us that we should remove barriers to good digital procurement, including unhelpful procurement rules which prevent NHS wide systems, and rebuild in house expertise in NHS digital teams, recruiting the best systems experts with cross-sector experience outside the NHS. This will give NHS digital teams both the choices and expertise they need to enable effective use of digital.
Giant 5: Education
“Some parents have been told that giving up their child into care is the only way that the child can be prioritised for a place at an appropriate school that meets their child’s SEN needs. Yet children going into care is extremely expensive, both in terms of the salary paid to foster carers, around £50k per year, and the large amount of a social worker’s time required to arrange it. This then reduces the amount of money available to meet SEN needs.”
Education is the final one of our Five Giants. We can see here that we need to prioritise rebuilding areas of education provision which existed in the original welfare state model in 1948 and up until austerity in 2010, particularly:
Local and effective school provision for children with special educational needs and disabilities (SEND), who often have their health issues exacerbated by having to travel longer distances to school. In some cases this is likely to have led to the early death of the child.
Provision of safe school buildings without RAAC concrete.
Reducing school attainment gaps for children from lower income families, children with a parent who does not speak English fluently, and some boys.
Health education in primary and secondary schools, including teaching children and young people how to cook low cost healthy meals and do DIY tasks to save money.
Rebuilding further education, adult education, and retraining of unemployed people.
Reviewing the need for degree courses for areas of health and social care where there are a lot of vacancies and people struggle to repay student loans, such as nursing and social work.
Education provision also needs to be updated for new requirements since 1948, particularly:
The need for free childcare now that the majority of women work.
The opportunity for digital to enable us to provide access to knowledge to a much wider audience, potentially making privileges like an Oxbridge education available to all, through, for example, the Open University offering recorded Oxbridge lectures on its free OpenLearn platform.
The Open University is also the best place to offer free online training for everyone in the Five Giants and Systems Thinking. This means all staff across Five Giants services, as well as service users, can benefit from this training. They can then put Systems Thinking into practice by using service user led Systems Thinking groups.
[i] https://www.goodreads.com/quotes/954454-there-comes-a-point-where-we-need-to-stop-just
[ii] https://www.amazon.co.uk/First-NHS-Tomleys-Modern-Healthcare/dp/1399038168
[iii] https://www.gov.uk/government/publications/independent-investigation-of-the-nhs-in-england
[iv] Donella Meadows, Thinking in Systems, 2008
[v] David Peter Stroh, Systems Thinking for Social Change, 2015
Download our report below:
Join us now
Become part of our educational think tank community.

